Laminitis can be defined as inflammation of the sensitive laminae of the foot.
In order to better understand the mechanism of laminitis it is important to have a basic knowledge of the anatomy of the equine foot.
The pedal bone (third phalanx) is completely contained inside the hoof capsule. On the inside of the hoof there are insensitive (epidermal) laminae that interlink with sensitive (dermal) laminae present on the surface of the pedal bone. The weight of the horse is taken by the incredibly strong interlocking of these structures.
The deep digital flexor tendon has it attachment on the palmar surface (back) of the pedal bone. When the tendon pulls on the pedal bone, the whole of the hoof capsule is drawn into flexion, achieving movement of the distal limb.
During Laminitis there is a breakdown of the connection between epidermal and dermal laminae.
As a result, vertical displacement (sinking) of the pedal bone or rotation may occur due to the pulling force of the deep digital flexor tendon.
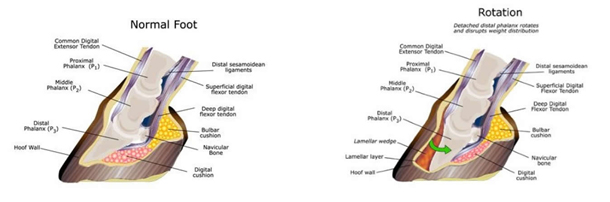
When rotation of the pedal bone occurs, abnormal pressure is applied to the sole, which becomes painful, especially at the toe.